PhalloBoards - An Online Community to Discuss Penile Girth Enhancement
Welcome, Guest |
Search Options
Search Results
| 07 Nov 2023 20:52 | |
|---|---|
Honestly, whatever Rejuvall recommends. They are a full-on Urology Practice, doing everything from buried penis, Peyronie's, penile injury/trauma, penis enlargement enlargement, and so on. Dr. Carney is also well respected in the field. Just listen to what they have to say and make your judgement call. From the sounds of it, I'd work on erectile function first before pursuing enlargement, because what good is a "big dick" if you can't use it? | |
| 28 Aug 2023 02:47 | |
|---|---|
Ellanse is a unique compound dermal filler that is not FDA approved. For this reason, its use would be an issue of legality, since it would NOT be permissible to use within the United States. Loria's Mystery Cocktail is also a unique compound dermal filler that is not FDA approved. For this reason, its use would be an issue of legality, since it would NOT be permissible to use within the United States. Comprendes? Do you know why the FDA regulates these fillers? To ensure they meet an acceptable risk threshold and are intended to provide positive benefits to the American patient/consumer. This is to test the efficacy of medical drugs and devices, which means Loria's Mystery Cocktail at BEST is unethical in its use(s), if not outright illegal. Also, I made clear numerous times that I couldn't prove he was injecting illegally, but that I was suspicious of it based on the information available (and elaborated on why). I did so clearly multiple times and here you are saying otherwise. Please READ. Call up any Cosmetic Clinic and ask them to read off their menu of fillers & other injectables. You'll hear Juvaderm, Bellafill, Botox, and so on. Not once are you going to hear, "and our In-House Specialty volume enhancer," like EVER. If they have Silikon1000, they'll inject you with just that. I mean again, nothing about this Loria smells right. Also are you telling me that he uses Silikon1000 (a brand-name) as a core ingredient in his patent, as well as the same ingredient that will be submitted to the FDA for approval? I'd be curious to see if Silikon1000 could sue in this instance, but the legality of this matter is admittedly above my pay-grade. Like if the perfect "mixture" constituted a high enough percentage of Silikon1000 so that it's effectively "Silikon1000-Lite", wouldn't this amount to some kind of infringement? Interesting to see where that goes (if it goes anywhere at all). You got duped by a "sleazy used car salesman" of a Doctor (no disrespect to any actual used car salesmen reading this lol) and you rather not swallow the pill. Every response you make falls flat on its face. You're not doing yourself or the Loria "brand" any justice to be frank, quit while you're ahead please. You claim you don't want to argue, but choose to anyways, all while making points that were previously refuted or addressed. Don't let this "ICU Nurse" thing get to your head buddy. And I was going to wait until later to publish this piece on the frontpage, but since I did mention lymphatics in a previous post, check out this article with a Urological insight on penile injections as well as a case follow-up on a penile & testicular silicone enhancement -- FRESH OFF THE PRESSES: Effectiveness of Silicone Injections for Penile Enlargements | |
| 25 Jan 2023 23:45 | |
|---|---|
The issue with fat-transfer are two factors: (1.) Its history. During the 2000s, fat-transfer was really the only filler option marketed since dermal fillers hadn't picked up in popularity for its use in the penis. During this time, many doctors would give the patient what they wanted, which often meant overfilling the shaft with high volumes of fat. Not surprisingly, this fat needs a blood supply to survive, and your body can vascularize the new tissue only so quickly, meaning excessive fat may and likely will die off. This explains why modern approaches to fat include layering it incrementally (like brick-laying) over multiple appointments to ensure sufficient blood supply, combining fat with other fillers, and/or the use of platelet rich plasma (PRP) to expedite the healing & vascularization process. (2.) The advent of filler alternatives. In the 2010s, new filler options were popping up, and much of their allure was that you wouldn't have harvest fat; this was especially noteworthy because you had to have sufficient amount of the right kind of fat the doctor would need for a successful result. You had the boom of PMMA in 2011, and the subsequent popularity of Ellanse and Hyaluronic Acid (HA) in the years that followed. Now that there are multiple options, fat-transfer ended up losing some of the phalloplasty market share. This is the answer to your why question. In my opinion, when performed by an experienced and qualified practitioner (which Rejuvall certainly are), fat-transfer is very much a viable option and its best attribute is that is your own tissue, likely making it the least prone to an adverse foreign body reaction (if at all). I hope that helps. | |
| 17 Feb 2022 22:07 | |
|---|---|
@donwfree Here is a response from Dr. Carney himself: Good question! I’m going to go the long way around the barn responding to your inquiry to address other questions I receive regarding lost size following installation of a penile prosthetic. Some History Regarding Penile Implants The first working prototype of an inflatable penile implant for severe erectile dysfunction was introduced by a urologist at Baylor named Brantley Scott, MD at the American Urology Association convention in New York City in 1973. It took another ten years for Dr. Brantley’s innovation to gain clearance from the FDA and become widely available. Four urologists were recruited to initially train other urologists on how to successfully install inflatable prosthetics for ED, including Rejuvall founder Steven L. Morganstern, MD. I’m including a photo from a TV talk show of this group including Dr. Morganstern, Brantley Scott, MD, John Mulcahy, MD, and Drago Montague, MD of the Cleveland Clinic. The biggest problem with early penile implant procedures was higher-than-expected rate of infections and formation of scar tissue. Renowned Urologist John Mulcahy, MD (seated third from the left in the attached photo), published what’s considered the gold standard for urologic surgeons regarding how not to trigger significant scar tissue or infection following implantation of a prosthetic. His solution was rooted in a tandem of key procedural insights plus accepting the fact a post-prosthesis erect penile would end up being about an inch shorter than it was before the implant was installed. Let’s fast forward to today’s times. The company Dr. Scott co-founded (AMS) is still the primary provider of inflatable implants in the world. Although various improvements have been made through the years, the core design is still fundamentally the same, which speaks volumes about Dr. Scott’s innovation. Two independent events helped shape the recent increase in patient complaints regarding lost size. Insurance companies began cutting the allowable reimbursement for penile implant procedures. It’s now less than one-third of what it used to be. Congruently, hospitals became more rigorous regarding the amount of allowable time for each procedure in their OR’s. The result seems to be that when an implanting urologist encounters a more complicated prosthetic case, the tandem of lower pay and hospital pressure triggers him/her to complete the operation based upon medical standards vs. penile length optimization. We encounter patients who claim they lost over three inches of erect length following installation of their implant. About eighty percent of the hospital procedures I personally perform for the university are repairs of failed surgical procedures. Thus, I’ve performed several replacements of penile prosthetic implants to regain lost length and learned a bit about what can be done to improve matters and what can’t. The unfortunate reality is that if a patient doesn’t get a new penile implant installed within six months following their initial procedure that resulted in significant loss of erect length, nothing can be done to reverse that outcome. An implant becomes firmly seated within the corpora over time and builds small amounts of scar tissue as it heals. This makes any further penile lengthening impossible. If we somehow added length to the penis through repositioning, the improved length would be floppy at the end of the penis and unable to penetrate. What can be done to improve lost size following a penile implant? The girth of the penis can be enhanced after the installation of a prosthetic implant. One pathway is non-surgical injection of a select hyaluronic (H/A) dermal filler. The other is transplanting your own fat within the subcutaneous tissues that surround the organ, assuming you’re a good candidate for fat tissue transplant. (Under the age of 63 (adipose cells begin to die as we age and won’t successfully transplant after a certain point); if diabetic, you must have an A1C of 7 or below; and you must be a non-smoker or have been completely off cigarettes for at least 90 days before your procedure). The hyaluronic pathway faces no health or age constrictions but has less longevity (usually about two years). Regarding your original question regarding using Ellansé as the bulking agent to improve girth, I don’t think that would be a good idea. The primary components of Ellansé are about 80% hydrocellulose and 20% polycaprolactone. Polycaprolactone is a fairly strong inflammatory agent that triggers production of Level I, II and III collagens about 24 hours after its first injection. The polycaprolactone could damage the walls of the inflatable implant and open the door to a host of medical complications. Given the fact your inflatable prosthetic can be damaged during a girth enhancement, I would recommend having a urologist perform the procedure because of their familiarity with the inner prosthetic design. It’s a somewhat time-consuming procedure to safely navigate around the implant when adding thickness. Another procedure some implant patients get is adding H/A to their glans to help restore lost rigidity. During installation of the prosthetic, about half of patients must have the unique blood supply to the glans severed during installation. This results in significant atrophy to the glans, hindering penetration. I always add about 3ML of Juvéderm Voluma to the glans during an implant enlargement for this reason. Finally, unlike a penile prosthesis, enhancement of a penile implant is considered a cosmetic procedure (elective) procedure and is never covered by insurance. Hope this information helps a bit for those looking to improve lost size following installation of a prosthetic penile implant. 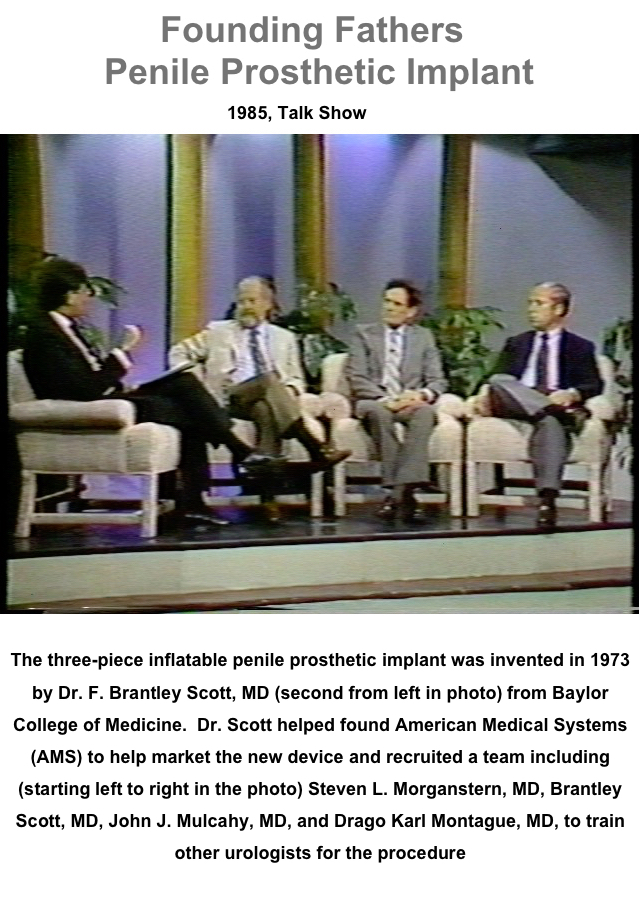  Category: Dr. Carney - Ask Me Questions Here | |
| 07 Aug 2021 14:37 | |
|---|---|
Dr. Carney works with Morganstern Urology (as well as their Rejuvall division which does male enhancement), and has performed a number of procedures for members of this forum. You can PM our Moderator @Texas who has seen the Doctor, or review reports found on this forum (as well as PMing other former patients). I also recommended them due to their proximity to you, but they'd likely be my first pick regardless, if I were facing potential complications from silicone. Also, on the 2.0 site, our Moderator Miracle8x7 ( phalloboards.websitetoolbox.com/post/mir...-5391236?&trail=1245 ) had revision work done with Dr. Carney & Dr. Morganstern on complications stemming from Silikon1000 injections although he has not updated in a while. It wouldn't hurt to message him on the old site, hopefully he'll check his inbox from time to time. I'm willing to wager the opinion of someone who's owned & operated a penis-enlargement forum for a decade might be the person whose recommendation is worth trusting - in other words, trust me Here are some doctors, including non-sponsors, ranked in who I'd personally see if I were in your shoes: Dr. Carney (and by extension, Dr. Morganstern; Georgia) Dr. Solomon (Pennsylvania) Dr. Alter (California) Dr. Gelman (California) Good luck. | |
| 16 Mar 2021 22:59 | |
|---|---|
HIGHLY unlikely that the weight of the fillers alone will have any significant impact on erect length, much less permanency of length. Flaccid can see improvement due to the fillers tendency to prohibit some retraction. Fillers vary in safety profiles and how long they last, see graphic below for some reference (you may need to click on it to scale the image to your screen). Your last question should be directed at Morgenstern's Clinic (here is contact info: www.rejuvall.com/ ) since it may depend on each individual's unique situation, but in general I suspect lengthening can be done even if you do have prior filler.  | |
| 14 Nov 2020 06:34 | |
|---|---|
I'd be very curious to track this practitioner down. Also, would be curious about the approach @morgansternrejuvall uses as they have an expensive glans option, and the photos look good. I read one study from a research hospital in Korea: It was for PE. Placement and volume in the PE case may also be different. Here's another Korea Study www.ncbi.nlm.nih.gov/pmc/articles/PMC6302150/ I am very impressed by the case study of this Urologist: www.urologicalcare.com/contents/penile-i...ns/penile-glans-size There is an excellent breakdown of details with photographs. | |

| 11 May 2020 11:39 | |
|---|---|
The following are community-generated questions that have been answered by representatives from Morganstern Rejuvall regarding their male enhancement services. If you'd like to submit your own question, please mail them to This email address is being protected from spambots. You need JavaScript enabled to view it. (1) PhalloBoards member "Chester" asks: "Hi Doctor, before I ask my question, I'm happy to report that the procedure has been a huge success. Thank you for your great work! My question has to do with the impact a filler in your penis has on blood pressure. There is only so much size and mass in the penis, and if you're adding filler volume, one stands to reason that there will be added pressure on the veins in the penis. I'm curious about your thoughts regarding long-term impact this has on blood pressure. I ask because, as we age, blood pressure tends to go up, and I think this topic is important yet rarely addressed. Personally I'm in my forties and there's a history of hypertension in my family, along with being pre-hypertensive." I’m happy to hear you’re pleased with your outcome Chester. When girth is added to the penis via any sort of injectable or FFT, that enhancement occurs by adding the bulking agent into to the subcutaneous tissue “surrounding” the vascularized penile organ. The incredibly small capillaries located within the subcutaneous tissue are not affected by total body blood pressure – they are simply too minuscule and remote to be impacted. If you added additional girth augmentation later, our limitation is the degree of stretch within that subcutaneous tissue – not the penis organ. Human tissue is very stretchable with time. You just can’t force stretch it without risks. Your erection process to attain a full engorgement is an automated sealing process within the organ. If you provided increased blood force it won’t change the amount of blood provided to the penis as it locks itself closed once a full dose of blood is in place for optimal penetration size. Alas, high blood pressure tends to cause an opposite effect on men and their erections as veins in the body can and will harden from high blood pressure, resulting in erectile dysfunction symptoms from insufficient arterial blood flow. Remember, your penis is located on the very edge of your body. That means it gets lower priority of blood flow when resources are limited – as with patients exhibiting cold hands and feet. Finally, some blood pressure medicines are notorious for triggering significant ED issues as they medicate the same sort of situation I just described. The hypertension drug we recommend patients not use for their blood pressure condition relative to penile performance is Propranolol. We’ve discovered it not only causes ED but also triggers penile fibrosis: the building block of Peyronie’s disease. (2) PhalloBoards member "Think" asks: "Texture / hardness is also a question ... I know I've been very happy with Ellanse in that regard, as have others with PMMA ... it feels really hard and natural when erect ... some have not with HA because it felt "squishy", although some have ... so how does FFT compare? More variable like HA?" FFT is almost identical to the feel of Ellanse in subsequent texture for the first couple of years after your augmentation. In years later as the augmented subcutaneous tissue stretches, it gets a little softer – but never as soft as H/A – unless...a patients receives multiple surgeries of FFT over time. Patients who add 2-3 inches of FFT girth with multiple procedures will often end up with a “squishy” hand when erect. I’m sure you’re already aware a female partner can’t detect a difference in the rigidity of the penile shaft – they only feel the variation in total measured girth. Most sex toys involving vaginal penetration in today's market have a softer outer finish for improved comfort. (3) PhalloBoards member "Kpk1435" asks (regarding Rejuvall's lengthening): "Do you know if it will be a horizontal cut or a VY log cut? I been thinking about lig cut for quite some time now but I can’t make up my mind because I am kind of worried about the angle drop. I searched online to see if there will be any before and after pics but can’t find none. Also do you know how much are they charging? If it is appropriate to ask such question here in the forum. I would greatly appreciate your response. Thank you." I’m going to provide a very lengthy response to your question in order to help you and others make the best possible decision for yourself in this regard. Let’s start with the ligaments themselves. Every guy has a different number, size, tautness and exact location of their suspensory ligaments. They were designed into men during a time of evolution when sex between human beings was often a very violent process. Keep in mind: we might like using our sexual organs for fun, but their sole purpose physiologically is the procreation of our species. Many, many, many years ago we needed a lot of structural support at the base of the penis in order to consummate sex. If we had sex like that nowadays we would probably be charged with a crime. What you “see” of your penis is where the organ becomes visible from underneath the pelvic bone. Your penis organ actually starts near the anus. The suspensory ligaments are connected to the base of the penis from the pelvic bone. There are actually four aspects to optimal penile lengthening. One, is the cutting of the ligaments at the base of the penis. The second is the release of the deep ligament. The third is repositioning as much of the penis organ that’s situated on the inside to an outward location as is safely possible. And finally, there’s stretching. It might be helpful to envision the suspensory ligaments at the base of the penis like the base roots you see around a tree in your front yard and the deep ligament as the tap root of that same tree. I bring this up because we see lots of patients who had a previous ligament release performed and complained they actually “lost” length. How could that happen? It happens because of patients seeking a minimized scar in achieving penile length. If we only cut the top suspensory ligaments (like the roots around the base of our imaginary tree) – the deep ligament (the tap root) will still hinder the penis from successful stretching. We found this most common for patients who had a ligament release performed through the scrotum to make it a “scar-less” procedure. Patients who had such procedures and are almost always unhappy with their length outcome are sometimes informed it’s likely “the ligament reattached”. However, we’ve discovered that wasn’t the case when we performed a subsequent lengthening surgery. The reason was rooted in the fact the deep ligament held fast and internal scar tissue underneath the skin from the procedure triggered new tautness and a reduction of penile length. While a VY-plasty is suitable for some patients, we found that we get the most optimal lengthening results via a 2-3-inch singular incision running straight up from the base of the penis at the pelvic bone. This opening allows optimal access the suspensory ligaments, the deep ligament and repositioning of the penis, as able. It’s important to understand that the penis doesn’t just “jump forward” following a release of the ligaments – they’re not that tight on 99% of patients. That’s why the penile repositioning is so important for most patients – along with the fact it inhibits the likelihood of ligament reattachment. It leaves a scar akin to a hernia operation which is what most single male patients use to describe where they got it in the future. The degree of work with stretching on the part of the patient following surgery is often under-amplified by some doctors but a crucial aspect of increased penile length. It starts 2-3 weeks after your procedure with a traction device that causes mild tension on the organ while it’s still healing from surgery. At this juncture, we want to inhibit any post-surgical retraction of the penis and loss of any of the hard-earned gains you enjoyed post-surgical. Tissue will naturally retract following any procedure and you want to make sure your penis doesn’t get involved in that process through mild traction. A couple of months later after things are completely healed, you’ll want to evolve to using weights to stretch the penis organ. Results from stretching are no longer inhibited by the strong ligaments you had cut for length. This program will trigger the cells to slightly tear and grow back larger over time – in a process similar to building muscle mass to your biceps. Alas, it’s time consuming. You need to stretch for two hours daily for six months after the procedure to achieve best results. The fear of a significant change in erect angle while standing up is most often promulgated by doctors who don’t perform penile lengthening procedures. The angle changes 5-20 degree’s depending upon your present angle when standing up straight. It drops more on a percentage basis if your engorgement points near straight upward and less if you’re presently situated me straight ahead. Most men are prone on a bed when erect and never notice that difference. A bigger consideration for some if the subsequent “looseness” at the base of the shaft following a ligament release. While most sexual positions are still fine in this state, the force of a partner coming down at an angle as with “cowgirl and reverse cowgirl” are challenging without putting your fingers at the base of the penis to add support. Thus, if “rodeo” sex is your favorite pastime, you need to think long and hard before considering a penile lengthening procedure. Thus, in summary: 1. You must have a ligament release in order to achieve real and lasting increase in penile length. 2. Only cutting the top ligaments to reduce scaring reduces the likelihood your lengthening will succeed. You need the deep ligament cut as well. 3. The post-surgical erect angle isn’t usually a big deal. The subsequent “looseness” at the base of the penis during rigorous sex is a more important consideration for some patients. 4. Stretching is required to achieve optimal results. If you’re not able or willing to invest the time in post-surgical stretching, it’s probably not worth your time and money to invest in a lengthening procedure. We presently charge $9,800 for our optimal lengthening procedure that includes release of top and deep ligaments plus penile repositioning, anesthesia and supporting stretching devices. Know that’s a lot of information but I hope it helps you make the best decision for your particular case. Dr. Carney Category: Dr. Carney - Ask Me Questions Here | |
| 06 Apr 2018 01:24 | |
|---|---|
I am choosing High and Tight circumcision style... You should not save money and choose the best doctor for this cosmetic surgery.. NO I am not get into PMMA cause my base erect girth is 6.5 inches and middle erect girth is 6.0 inches circumference. I am looking for detachment/cut for length with Dr Morganstern in Atlanta in the near future. morgansternhealth.com/penile-enlargement/ www.rejuvall.com/rejuvall-penis-enlargem...halloplasty-surgery/ Attn.: I am still waiting for some positive review before I schedule a consultation with Dr Morganstern. | |
